Can I Continue Taking Multivitamins if I m Taking Prevacid
US Pharm. 2007;1:42-55.
Vitamins and minerals serve crucial functions in almost all bodily processes and must be obtained from foods or supplements, as our bodies are unable to make them. According to results of the National Health and Nutrition Examination Survey, 52% of adults take dietary supplements.1 Supplement use is typically a safe and effective method of maintaining a healthy body; however, supplements have the potential to interact with prescribed medications. In this article, common drug interactions with vitamins and minerals are discussed, along with suggestions on how the pharmacist should manage these interactions.
It is important for pharmacists to be able to identify patients who are most at risk. Risk factors for poor outcomes from drug interactions include use of multiple medications and/or supplements, older age, inadequate kidney or liver function, and the use of medications with narrow therapeutic indexes. Patients with these risk factors should be targeted for interventions to prevent drug interactions with vitamins and minerals.
When managing interactions between medications and vitamin/mineral supplements, the pharmacist has several factors to keep in mind. First, he or she needs to determine the need for the supplement during the time the medication is to be taken. For a short course of medication, it is usually possible to discontinue the supplement until the therapy is completed. Second, the pharmacist should identify alternatives. For example, if the interacting substance comes from an antacid that the patient needs to treat symptoms of gastroesophageal reflux disease, an alternative such as an H2-blocker or proton pump inhibitor can be used during the course of the medication. If the affected medication is to be taken chronically, and the supplement is deemed necessary, the pharmacist should work with the patient and the prescriber to suggest alternatives that would limit exposure to potentially dangerous drug interactions.
Vitamins and Drug Interactions
Vitamin A: Vitamin A is a fat-soluble vitamin found in everyday foods, including liver, yellow-orange fruits and vegetables such as carrots, margarine, milk, and dark green, leafy vegetables such as spinach. It is not commonly available as a supplement on its own; however, it can be found as a component of multivitamins and combination supplements targeted towards improving skin, hair, and nails. Vitamin A plays an important role in vision, bone growth, cell differentiation, and the immune system. Vitamin A deficiency often leads to problems with eyesight, a situation less common in the United States than in underdeveloped countries where nutrition may be poor. Some conditions such as celiac disease, Crohn's disease, and pancreatic disorders may lead to malabsorption of vitamin A from the diet.
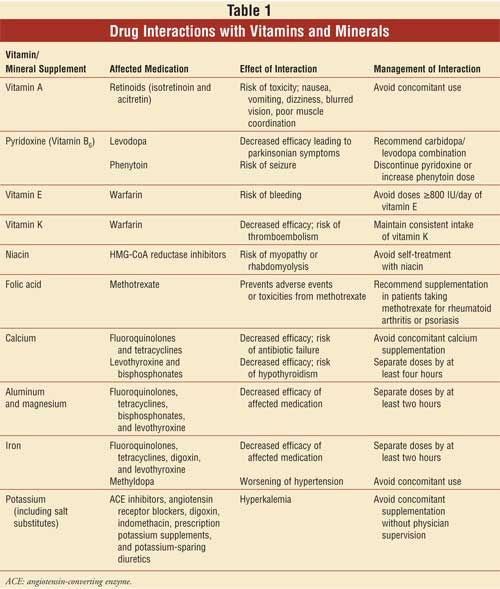
Interactions with vitamin A become a concern with the use of products classified as retinoids--compounds that are chemically similar to vitamin A. Retinoids such as isotretinoin (Accutane) and acitretin (Soriatane) are indicated for the treatment of acne and psoriasis, respectively. When retinoid products are prescribed, there is concern of vitamin A toxicity.2 Pharmacists should alert patients who are taking retinoid products to the importance of avoiding excess vitamin A. They should also educate patients about the signs and symptoms of vitamin A toxicity, such as nausea, vomiting, dizziness, blurred vision, and poor muscle coordination.
Vitamin B6 (Pyridoxine):
Vitamin B6, or pyridoxine, is a water-soluble vitamin used to treat deficiencies in vitamin B6 and some types of anemia. Foods rich in pyridoxine include meats, whole grains, and certain fruits and vegetables. Pyridoxine has been shown to decrease the effects of both phenytoin and levodopa. However, this effect is not seen when levodopa is prescribed in combination with carbidopa, which prevents the interaction from occurring. In the rare instance that patients are taking levodopa in absence of carbidopa, pharmacists should advise their patients to avoid any products containing pyridoxine, because even smaller doses, such as 10 to 25 mg of pyridoxine, may be enough to inhibit levodopa.3 Pharmacists should strongly encourage the switch to a levodopa/carbidopa combination product if a patient is not already taking this combination therapy.
There is limited evidence that high doses of pyridoxine reduce phenytoin serum concentrations, thereby reducing the efficacy of phenytoin. One study of patients with seizure disorders found an association between pyridoxine 200 mg/day and reductions in phenytoin concentration of nearly 50%.4 Effects of pyridoxine doses lower than 200 mg/day on phenytoin serum concentration have not been established; however, lower doses can be considered if someone taking a multivitamin presents with low phenytoin serum concentrations. In these instances, it may be necessary to discontinue or lower the dosage of the multivitamin or to increase the dosage of phenytoin.
Vitamin E:
Vitamin E is a fat-soluble vitamin that is used in an array of ailments, including vitamin E deficiency, atherosclerosis, Alzheimer's disease, and various cancers. It is also a common supplement taken by patients with cardiovascular disease. Case reports have documented an increased risk of bleeding in patients taking vitamin E and warfarin concomitantly. This adverse effect is more likely to occur with larger doses of vitamin E (>800 IU) rather than smaller doses found in multivitamins.5,6 Therefore, pharmacists should advise patients taking warfarin to take a multivitamin for their daily source of vitamin E rather than a supplement containing only vitamin E.
There is controversy over vitamin E and other antioxidants with respect to chemotherapy. A theoretical interaction has been proposed whereby antioxidants interfere with the oxidative mechanism of the chemotherapeutic agent, thereby reducing its effectiveness. The clinical implications of this interaction is still unknown; but it might be worthwhile, until more is known, to counsel patients about avoiding antioxidant supplements while undergoing chemotherapy treatments that rely on this mechanism. However, it is important to note that antioxidants are sometimes used to prevent or lessen the toxic effects of specific agents. Patients on chemotherapy should be counseled not to supplement on their own and to inform their oncologist of all dietary supplements and alternative therapies.7
Vitamin K:
Vitamin K is indicated to reverse supratherapeutic international normalized ratio (INR) caused by warfarin. When warfarin and vitamin K–containing products are taken together, the activity of warfarin is decreased and results in a decreased prothrombin time and INR.8 This puts the patient at risk for suboptimal anticoagulation, possibly leading to thromboembolic events such as deep venous thrombosis, pulmonary embolism, myocardial infarction, or stroke. Vitamin K is obtained from the diet through green, leafy vegetables such as spinach and broccoli. Pharmacists should advise all patients taking warfarin to eat consistent diets of green, leafy vegetables and avoid inconsistent use of supplements that contain vitamin K (i.e., patients should not routinely change their intake of vitamin K–containing supplements).
Niacin:
Niacin is a B-complex vitamin used for the treatment of hyperlipidemia and pellagra. Patients may try to self-treat high cholesterol with a niacin supplement. The combination of niacin and HMG-CoA reductase inhibitors (statins) may increase the risk of myopathies or rhabdomyolysis.9,10 Pharmacists are likely to encounter this interaction, since statins are among the most commonly prescribed medications. The use of niacin with statins should be recommended only if the benefits of lipid-lowering outweigh the risks of myopathies and rhabdomyolysis. Typically, the interaction occurs at doses of 1 g/day or greater of niacin. Generally, over-the-counter niacin supplements are not supplied in doses this high. Pharmacists should encourage patients to take niacin supplements only under the supervision of a physician.
Folic Acid:
Folic acid is a B-complex vitamin used to treat and prevent folic acid deficiency. Folic acid supplementation is commonly recommended during methotrexate therapy as prophylaxis against toxicities in patients with rheumatoid arthritis and psoriasis. Folic acid deficiency is common in these patients, since methotrexate inhibits dihydrofolate reductase (an enzyme that reduces dihydrofolic acid to tetrahydrofolic acid).11 Once metabolized to tetrahydrofolate, folic acid aids in multiple biochemical processes to synthesize DNA, RNA, and various proteins. Studies have shown that folic acid supplementation reduces toxicities of methotrexate without affecting efficacy in long-term, low-dose methotrexate therapy for rheumatoid arthritis or psoriasis. Pharmacists should recommend folic acid supplementation in patients prescribed methotrexate for rheumatoid arthritis or psoriasis, especially if adverse effects or toxicities, such as abnormalities in blood cell counts and varying degrees of mucositis and diarrhea, are present. However, it is important to note that some evidence suggests that folic acid reduces the efficacy of methotrexate in cancer therapy.12
Folic acid has also been reported to decrease the efficacy of phenytoin, but only at doses 5 mg/day or greater, which would be an unlikely dose for supplementation with over-the-counter products.13
Minerals and Drug Interactions
Calcium: Calcium is a mineral supplement taken primarily to prevent or treat osteoporosis. It is found in dairy products and is available as a supplement or as a component of some antacids, such as Tums. One study determined that 67% of women and 25% of men take a calcium supplement regularly; because calcium is associated with significant drug interactions, pharmacists should question their patients about calcium intake.14
Calcium interacts with prescription medications by limiting their absorption through chelation. Significant interactions have been observed between calcium and certain antibiotics--namely tetracyclines and fluoroquinolones. Calcium carbonate can reduce the bioavailability of ciprofloxacin by 40%, which could result in inadequate infection treatment and increased complications.15 Patients taking tetracyclines or fluoroquinolones should avoid the supplement altogether during the course of therapy, which is usually a short period of time.16,17
Typically, pharmacists will instruct patients to space the doses of medications and/or supplements whose absorption is affected by binding. Controversy, however, exists on how much time is long enough to wait between doses. A minimum of two hours is usually mandated, with some sources citing four to six hours as a minimum recommendation. For example, it is recommended that doses of calcium and levothyroxine be separated by at least four hours, because the former decreases the bioavailability of the latter.18
In addition, it is important to note that several medications, when used chronically, can affect the body's utilization of calcium. Corticosteroids decrease the absorption of calcium, which, over time, can lead to osteoporosis. Loop diuretics increase the excretion of calcium, while drugs that affect vitamin D (which promotes of calcium absorption), such as phenytoin, phenobarbital, and orlistat, may decrease the amount of calcium absorbed from the diet.19 Patients taking these medications could benefit from a calcium supplement, especially one containing vitamin D. Pharmacists are in a key position to speak with patients taking these medications and to recommend adequate calcium intake and supplementation, particularly for patients with other risk factors for osteoporosis.
Aluminum and Magnesium:
Aluminum and magnesium are unlikely to be used solely as supplements; however, they are found in common over-the-counter antacid products. Like calcium, they can bind to vulnerable medications, decreasing their bioavailability and lessening their efficacy. Fluoroquinolone and tetracycline antibiotics, bisphosphonates, and levothyroxine may be affected by aluminum and magnesium; therefore, doses of these drugs should not be taken within two hours of aluminum or magnesium consumption. If the patient is not responding to therapy as expected, the pharmacist should recommend that the aluminum or magnesium product be discontinued and an alternative identified.
Iron:
Iron supplements are needed if the body cannot produce a sufficient amount of red blood cells. Lack of iron may lead to tiredness, shortness of breath, decreases in physical performance, learning problems, and an increased risk of infection.
Patients taking iron supplements or multivitamins that contain iron should be instructed to avoid taking their supplement within two hours of a dose of tetracycline or fluoroquinolone antibiotics, digoxin, or levothyroxine.20,21 In addition, patients taking both calcium and iron supplements should be informed that because these supplements compete for absorption, they should be dosed at different times of the day.
Iron salts can also interfere with the absorption of levodopa, decreasing peak levels by 55% and area under the curve by 51%.20 If the patient is experiencing breakthrough parkinsonian symptoms, iron should be avoided. If this is not possible, the dose of the levodopa should be increased. Iron can also cause worsening of hypertension in patients taking methyldopa, and concomitant administration is not recommended.22
The absorption of iron can be affected by gastric acidity, and a fair amount of evidence exists to support limited iron absorption in patients taking proton pump inhibitors and medications that decrease gastric acidity.23-26 In iron-deficient patients who require proton pump inhibitors, intravenous administration of iron is recommended. Interactions between iron and omeprazole, which was recently switched to over-the-counter status, may not be easily identifiable; therefore, pharmacists should question patients about their consumption of omeprazole and iron supplements.
Potassium:
Although most patients taking potassium supplementation receive this mineral in the form of a prescription product, some over-the-counter products contain potassium. Any medication that increases potassium levels in the body has the potential to interact with supplemental potassium. Patients should use caution when taking extra potassium if they take any of the following prescription medications: angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, digoxin, indomethacin, prescription potassium supplements, and the potassium-sparing diuretics triamterene or spironolactone. While the amount of potassium found in over-the-counter vitamin and mineral supplements is unlikely to cause major interactions, the pharmacist should warn patients of the potential for interaction, particularly if the patient is at risk for renal insufficiency. When counseling patients about the importance of avoiding excess potassium, pharmacists should mention that most common salt substitutes available in supermarkets contain potassium; therefore, these products should be avoided in patients at risk for hyperkalemia. Salt substitutes contain significantly higher amounts of potassium than do combination vitamin/mineral supplements sold over-the-counter. For example, a 1/4-teaspoon serving of NoSalt provides 650 mg of potassium. Considering that a 20-mEq prescription tablet contains 780 mg of potassium, a patient can easily accumulate potassium if using a salt substitute and thus should be warned against consuming these products if taking medications that retain potassium.
Conclusion
There are many different types of drug interactions with vitamins and minerals, ranging in severity and significance. Patients may not think to share information with their pharmacist about the vitamins and minerals they take, or they may feel the substances are harmless and irrelevant to their medication regimen. Because of the likelihood of an interaction, pharmacists should question patients not only about the drug allergies they have but also about the vitamins and minerals they ingest daily. Although this article did not discuss herbal products and other nutraceuticals, use of these products is important to document as well. Without this information, pharmacists cannot provide the necessary screening for interactions. Information about the use of vitamins, minerals, herbal products, and other nutraceuticals should be documented in patients' records for future reference. In addition, pharmacists should encourage software vendors and employers to provide fields in their profile systems for over-the-counter medications and supplements, since these products can impact care and cause easily avoidable drug interactions that could put the patient at risk for poor outcomes or adverse effects.
REFERENCES
1. Radimer K, Bindewald B, Hughes J, et al. Dietary supplement use by US adults: data from the National Health and Nutrition Examination Survey, 1999–2000. Am J Epidemiol. 2004;160:339-349.
2. Dietary Supplement Fact Sheet: Vitamin A and Carotenoids. Bethesda, MD: National Institutes of Health: Office of Dietary Supplements; 2005.
3. Leon AS, Spiegel HE, Thomas G, Abrams WB. Pyridoxine antagonism of levodopa in parkinsonism. JAMA. 1971;218:1924-1927.
4. Hansson O, Sillanpaa M. Letter: Pyridoxine and serum concentrations of phenytoin and phenobarbitone. Lancet . 1976;1:256.
5. Corrigan JJ Jr, Marcus FI. Coagulopathy associated with vitamin E ingestion. JAMA. 1974;230:1300-1301.
6. Schrogie JJ. Coagulopathy and fat-soluble vitamins. JAMA. 1975;232:19.
7. Conklin KA. Dietary antioxidants during cancer chemotherapy: impact on chemotherapeutic effectiveness and development of side effects. Nutr Cancer. 2000;37(1):1-18.
8. Greenblatt DJ, von Moltke LL. Interaction of warfarin with drugs, natural substances, and foods. J Clin Pharmacol. 2005;45:127-132.
9. Cooke HM. Lovastatin- and niacin-induced rhabdomyolysis. Hosp Pharm. 1994;29:33-34.
10. Malloy MJ, Kane JP, Kunitake ST, Tun P. Complementarity of colestipol, niacin, and lovastatin in treatment of severe familial hyper cholesterolemia. Ann Intern Med. 1987;107:616-623.
11. Endresen GK, Husby G. Folate supplementation during methotrexate treatment of patients with rheumatoid arthritis. An update and proposals for guidelines. Scand J Rheumatol. 2001;30:129-134.
12. Drugs & Supplements. Folate (folic acid). Bethesda, MD: National Library of Medicine (US); 2005.
13. MacCosbe PE, Toomey K. Interaction of phenytoin and folic acid. Clin Pharm. 1983;2:362-369.
14. Dawson-Hughes B, Harris SS, Dallal GE, et al. Calcium supplement and bone medication use in a US Medicare health maintenance organization. Osteoporos Int. 2002;13:657-662.
15. Frost RW, Lettieri JT, Noe A, et al. Effect of aluminum hydroxide and calcium carbonate antacids on ciprofloxacin bioavailability. Clin Pharmacol Ther. 1989a;45:165.
16. Product Information: Vibramycin, doxycycline. Pfizer Laboratories, New York, NY, 1990.
17. Product Information: Cipro, ciprofloxacin. Bayer Corporation, West Haven, CT, 2002.
18. Product Information: Synthroid, levothyroxine. Oral tablet, USP, levothyroxine sodium oral tablet, USP. Abbott Laboratories, North Chicago, IL, 2002.
19. Greenberger NJ. Absorption of tetracyclines: interference by iron. Ann Intern Med. 1971;74:792-793.
20. Jellin JM, Batz F, Hitchens K. Pharmacist's Letter/Prescriber's Letter Natural Medicines Comprehensive Database. 2nd ed. Stockton, CA: Therapeutic Research Faculty; 1999:1241-1249.
21. Campbell NR, Hasinoff BB, Stalts H, et al. Ferrous sulfate reduces thyroxine efficacy in patients with hypothyroidism. Ann Intern Med. 1992;117:1010-1013.
22. Campbell NR, Hasinoff B. Ferrous sulfate reduces levodopa bioavailability: chelation as a possible mechanism. Clin Pharmacol Ther. 1989;45:220-225.
23. Campbell N, Paddock V, Sundaram R. Alteration of methyldopa absorption, metabolism, and blood pressure control caused by ferrous sulfate and ferrous gluconate. Clin Pharmacol Ther. 1988;43:381-386.
24. Product Information: Prilosec, omeprazole. Astra Merck Inc., Wayne, PA, 1995.
25. Sharma VR, Brannon MA, Carloss EA. Effect of omeprazole on oral iron replacement in patients with iron deficiency anemia. South Med J. 2004;97:887-889.
26. Product Information: Prevacid, lansoprazole. TAP Pharmaceuticals, Lake Forest, IL, 2002.
To comment on this article, contact editor@uspharmacist.com.
Source: https://www.uspharmacist.com/article/drug-interactions-with-vitamins-and-minerals
0 Response to "Can I Continue Taking Multivitamins if I m Taking Prevacid"
Post a Comment